

Latest news
Browse Now The Latest News, Medical And Scientific Explorations And New Devices














Recent Posts


May 3, 2025

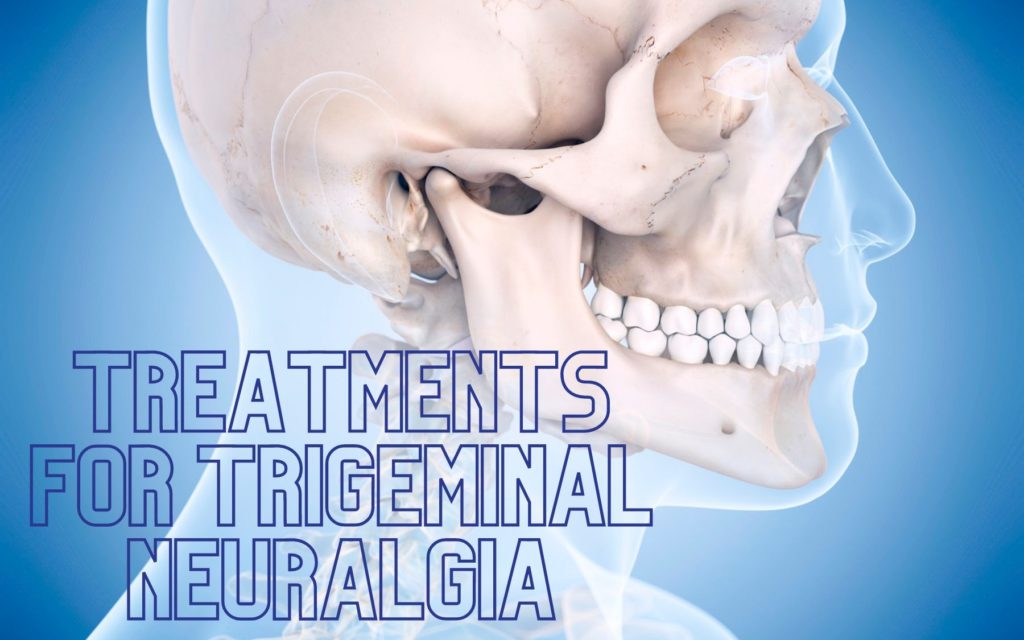
Trigeminal neuralgia (TN), also known as tic douloureux, is sometimes described as the most excruciating pain known to humanity. The pain typically involves the lower face and jaw, although sometimes it affects the area around the nose and above the eye. This intense, stabbing, electric shock-like pain is caused by irritation of the trigeminal nerve, which sends branches to the forehead, cheek and lower jaw. It usually is limited to one side of the face. The pain can be triggered by an action as routine and minor as brushing your teeth, eating or the wind. Attacks may begin mild and short, but if left untreated, trigeminal neuralgia can progressively worsen.
Although trigeminal neuralgia cannot always be cured, there are treatments available to alleviate the debilitating pain. Normally, anticonvulsive medications are the first treatment choice. Surgery can be an effective option for those who become unresponsive to medications or for those who suffer serious side effects from the medications.
What is The Trigeminal Nerve
The trigeminal nerve is one set of the cranial nerves in the head. It is the nerve responsible for providing sensation to the face. One trigeminal nerve runs to the right side of the head, while the other runs to the left. Each of these nerves has three distinct branches. “Trigeminal” derives from the Latin word “tria,” which means three, and “geminus,” which means twin. After the trigeminal nerve leaves the brain and travels inside the skull, it divides into three smaller branches, controlling sensations throughout the face:
Ophthalmic Nerve (V1): The first branch controls sensation in a person’s eye, upper eyelid and forehead.
Maxillary Nerve (V2): The second branch controls sensation in the lower eyelid, cheek, nostril, upper lip and upper gum.
Mandibular Nerve (V3): The third branch controls sensations in the jaw, lower lip, lower gum and some of the muscles used for chewing.
Prevalence and Incidence
It is reported that 150,000 people are diagnosed with trigeminal neuralgia (TN) every year. While the disorder can occur at any age, it is most common in people over the age of 50. The National Institute of Neurological Disorders and Stroke (NINDS) notes that TN is twice as common in women than in men. A form of TN is associated with multiple sclerosis (MS).
Causes of Trigeminal Neuralgia
There are two types of TN — primary and secondary. The exact cause of TN is still unknown, but the pain associated with it represents an irritation of the nerve. Primary trigeminal neuralgia has been linked to the compression of the nerve, typically in the base of the head where the brain meets the spinal cord. This is usually due to contact between a healthy artery or vein and the trigeminal nerve at the base of the brain. This places pressure on the nerve as it enters the brain and causes the nerve to misfire. Secondary TN is caused by pressure on the nerve from a tumor, MS, a cyst, facial injury or another medical condition that damages the myelin sheaths.
Symptoms
Most patients report that their pain begins spontaneously and seemingly out of nowhere. Other patients say their pain follows a car accident, a blow to the face or dental work. In the cases of dental work, it is more likely that the disorder was already developing and then caused the initial symptoms to be triggered. Pain often is first experienced along the upper or lower jaw, so many patients assume they have a dental abscess. Some patients see their dentists and actually have a root canal performed, which inevitably brings no relief. When the pain persists, patients realize the problem is not dental-related.
The pain of TN is defined as either type 1 (TN1) or type 2 (TN2). TN1 is characterized by intensely sharp, throbbing, sporadic, burning or shock-like pain around the eyes, lips, nose, jaw, forehead and scalp. TN1 can get worse resulting in more pain spells that last longer. TN2 pain often is present as a constant, burning, aching and may also have stabbing less intense than TN1.
TN tends to run in cycles. Patients often suffer long stretches of frequent attacks, followed by weeks, months or even years of little or no pain. The usual pattern, however, is for the attacks to intensify over time with shorter pain-free periods. Some patients suffer less than one attack a day, while others experience a dozen or more every hour. The pain typically begins with a sensation of electrical shocks that culminates in an excruciating stabbing pain within less than 20 seconds. The pain often leaves patients with uncontrollable facial twitching, which is why the disorder is also known as tic douloureux.
Pain can be focused in one spot or it can spread throughout the face. Typically, it is only on one side of the face; however, in rare occasions and sometimes when associated with multiple sclerosis, patients may feel pain in both sides of their face. Pain areas include the cheeks, jaw, teeth, gums, lips, eyes and forehead.
Trigeminal Neuralgia triggered by the following:
1. Touching the skin lightly
2. Washing
3. Shaving
4. Brushing teeth
5. Blowing the nose
6. Drinking hot or cold beverages
7. Encountering a light breeze
8. Applying makeup
9. Smiling
10. Talking
The symptoms of several pain disorders are similar to those of trigeminal neuralgia. The most common mimicker of TN is trigeminal neuropathic pain (TNP). TNP results from an injury or damage to the trigeminal nerve. TNP pain is generally described as being constant, dull and burning. Attacks of sharp pain can also occur, commonly triggered by touch. Additional mimickers include:
1. Temporal tendinitis
2. Ernest syndrome (injury of the stylomandibular ligament
3. Occipital neuralgia
4. Cluster headaches/ migraines
5. Giant cell arteritis
6. Dental pain
7. Post-herpetic neuralgia
8. Glossopharyngeal neuralgia
9. Sinus infection
10. Ear infection
11. Temporomandibular joint syndrome (TMJ)
12. Diagnosis
TN can be very difficult to diagnose, because there are no specific diagnostic tests and symptoms are very similar to other facial pain disorders. Therefore, it is important to seek medical care when feeling unusual, sharp pain around the eyes, lips, nose, jaw, forehead and scalp, especially if you have not had dental or other facial surgery recently. The patient should begin by addressing the problem with their primary care physician. They may refer the patient to a specialist later.
How to test Trigeminal Neuralgia
Magnetic resonance imaging (MRI) can detect if a tumor or MS is affecting the trigeminal nerve. A high-resolution, thin-slice or three-dimensional MRI can reveal if there is compression caused by a blood vessel. Newer scanning techniques can show if a vessel is pressing on the nerve and may even show the degree of compression. Compression due to veins is not as easily identified on these scans. Tests can help rule out other causes of facial disorders. TN usually is diagnosed based on the description of the symptoms provided by the patient, detailed patient history and clinical evaluation. There are no specific diagnostic tests for TN, so physicians must rely heavily on symptoms and history. Physicians base their diagnosis on the type pain (sudden, quick and shock-like), the location of the pain and things that trigger the pain. Physical and neurological examinations may also be done in which the doctor will touch and examine parts of your face to better understand where the pain is located.
Treatments of Trigeminal Neuralgia
Non-Surgical Treatments
There are several effective ways to alleviate the pain, including a variety of medications. Medications are generally started at low doses and increased gradually based on patient’s response to the drug.
Carbamazepine, an anticonvulsant drug, is the most common medication that doctors use to treat TN. In the early stages of the disease, carbamazepine controls pain for most people. When a patient shows no relief from this medication, a physician has cause to doubt whether TN is present. However, the effectiveness of carbamazepine decreases over time. Possible side effects include dizziness, double vision, drowsiness and nausea.
Gabapentin, an anticonvulsant drug, which is most commonly used to treat epilepsy or migraines can also treat TN. Side effects of this drug are minor and include dizziness and/or drowsiness which go away on their own.
Oxcarbazepine, a newer medication, has been used more recently as the first line of treatment. It is structurally related to carbamazepine and may be preferred, because it generally has fewer side effects. Possible side effects include dizziness and double vision.
Other medications include: baclofen, amitriptyline, nortriptyline, pregabalin, phenytoin, valproic acid, clonazepam, sodium valporate, lamotrigine, topiramate, phenytoin and opioids.
There are drawbacks to these medications, other than side effects. Some patients may need relatively high doses to alleviate the pain, and the side effects can become more pronounced at higher doses. Anticonvulsant drugs may lose their effectiveness over time. Some patients may need a higher dose to reduce the pain or a second anticonvulsant, which can lead to adverse drug reactions. Many of these drugs can have a toxic effect on some patients, particularly people with a history of bone marrow suppression and kidney and liver toxicity. These patients must have their blood monitored to ensure their safety.
Surgery Treatment
If medications have proven ineffective in treating TN, several surgical procedures may help control the pain. Surgical treatment is divided into two categories: 1) open cranial surgery or 2) lesioning procedures. In general, open surgery is performed for patients found to have pressure on the trigeminal nerve from a nearby blood vessel, which can be diagnosed with imaging of the brain, such as a special MRI. This surgery is thought to take away the underlying problem causing the TN. In contrast, lesioning procedures include interventions that injure the trigeminal nerve on purpose, in order to prevent the nerve from delivering pain to the face. The effects of lesioning may be shorter lasting and in some keys may result in numbness to the face.
Open Surgery
Microvascular decompression involves microsurgical exposure of the trigeminal nerve root, identification of a blood vessel that may be compressing the nerve and gentle movement of the blood vessel away from the point of compression. Decompression may reduce sensitivity and allow the trigeminal nerve to recover and return to a more normal, pain-free condition. While this generally is the most effective surgery, it also is the most invasive, because it requires opening the skull through a craniotomy. There is a small risk of decreased hearing, facial weakness, facial numbness, double vision, stroke or death.
Lesioning Procedures
Percutaneous radiofrequency rhizotomy treats TN through the use of electrocoagulation (heat). It can relieve nerve pain by destroying the part of the nerve that causes pain and suppressing the pain signal to the brain. The surgeon passes a hollow needle through the cheek into the trigeminal nerve. A heating current, which is passed through an electrode, destroys some of the nerve fibers.
Percutaneous balloon compression utilizes a needle that is passed through the cheek to the trigeminal nerve. The neurosurgeon places a balloon in the trigeminal nerve through a catheter. The balloon is inflated where fibers produce pain. The balloon compresses the nerve, injuring the pain-causing fibers, and is then removed.
Percutaneous glycerol rhizotomy utilizes glycerol injected through a needle into the area where the nerve divides into three main branches. The goal is to damage the nerve selectively in order to interfere with the transmission of the pain signals to the brain.
Stereotactic radiosurgery (through such procedures as Gamma Knife, Cyberknife, Linear Accelerator (LINAC) delivers a single highly concentrated dose of ionizing radiation to a small, precise target at the trigeminal nerve root. This treatment is noninvasive and avoids many of the risks and complications of open surgery and other treatments. Over a period of time and as a result of radiation exposure, the slow formation of a lesion in the nerve interrupts transmission of pain signals to the brain.
Overall, the benefits of surgery or lesioning techniques should always be weighed carefully against its risks. Although a large percentage of TN patients report pain relief after procedures, there is no guarantee that they will help every individual.
Neuromodulation
For patients with TNP, another surgical procedure can be done that includes placement of one or more electrodes in the soft tissue near the nerves, under the skull on the covering of the brain and sometimes deeper into the brain, to deliver electrical stimulation to the part of the brain responsible for sensation of the face. In peripheral nerve stimulation, the leads are placed under the skin on branches of the trigeminal nerve. In motor cortex stimulation (MCS), the area which innervates the face is stimulated. In deep brain stimulation (DBS), regions that affect sensation pathways to the face may be stimulated.
How to Prepare for a Neurosurgical Appointment
Write down symptoms. This should include: What the pain feels like (for example, is it sharp, shooting, aching, burning or other), where exactly the pain is located (lower jaw, cheek, eye/forehead), if it is accompanied by other symptoms (headache, numbness, facial spasms), duration of pain (weeks, months, years), pain-free intervals (longest period of time without pain or in between episodes), severity of pain (0=no pain, 10=worst pain)
Note any triggers of pain (e.g. brushing teeth, touching face, cold air)
Make a list of medications and surgeries related to the face pain (prior medications, did they work, were there side effects), current medications (duration and dose)
Write down questions in advance
Understand that the diagnosis and treatment process for TN is not simple. Having realistic expectations can greatly improve overall outcomes.
Follow-up
Patients should follow-up with their primary care providers and specialists regularly to maintain their treatment. Typically, neuromodulation surgical patients are asked to return to the clinic every few months in the year following the surgery. During these visits, they may adjust the stimulation settings and assess the patient’s recovery from surgery. Routinely following-up with a doctor ensures that the care is correct and effective. Patients who undergo any form of neurostimulation surgery will also follow-up with a device representative who will adjust the device settings and parameters as needed alongside their doctors.

In the realm of urologic procedures, a noteworthy shift is taking place, and it’s all about conscious sedation. Canadian researchers have delved into the realm of conscious sedation as an attractive alternative to general anesthesia, and the results are remarkable.
Patient preference for Conscious Sedation:
Patients undergoing various urologic procedures, including endourologic, ureteric, urethral, and advanced cystoscopic interventions, have made their voices heard. A majority of these patients expressed a distinct preference for conscious sedation, even when given the choice to be fully awake during the procedure. Kapilan Panchendrabose, MSc, a medical student from the University of Manitoba in Winnipeg, Manitoba, Canada, presented these findings at the European Association of Urology (EAU) 2022 Annual Meeting.
Traditionally, the standard approach for most urologic procedures has been to administer general or spinal anesthesia to patients. However, this approach comes with its fair share of risks, including adverse side effects, increased costs, and longer operating room wait times. Conscious sedation, offering anesthetic and analgesic relief during certain urologic procedures, provides a promising solution.
Expanding the Technique by Studying Details
The University of Manitoba researchers initially explored conscious sedation for the treatment of ureteric calculi and expanded this technique to include various advanced urologic procedures. Their hypothesis was straightforward: patients under conscious sedation would not only tolerate the procedure but would also prefer it to general anesthesia for subsequent surgeries.
Their prospective, nonrandomized cohort study, conducted from June through August 2021, included rigid and flexible ureteroscopy, ureteric stent insertions/exchanges, scrotal/penile procedures (such as hydroceles and testicular biopsies), urethral dilations, and advanced cystoscopic procedures (including bladder biopsies and botox therapy). These procedures were performed with sedation using fentanyl, midazolam, or both agents.
The study outcomes were highly promising. With a success rate of 96.5% and no intraoperative complications, conscious sedation emerged as a safe and effective choice for urologic procedures. Even more compelling, 85% of patients, out of the 161 who completed post-procedure questionnaires four to six weeks later, expressed a strong preference for conscious sedation if they were to undergo a similar procedure in the future.
Factors influencing the choice of conscious sedation
When it comes to the factors influencing the choice of conscious sedation over general anesthesia, age played a role, with older patients showing a greater preference. Additionally, the surgeon’s perception of the patient’s tolerability during the procedure had an impact.
In a multivariate analysis, other variables such as body mass index, gender, prior conscious sedation experience, Charlson comorbidity index, procedure type, drug type, and time of the procedure did not predict the choice of anesthesia.
Kapilan Panchendrabose emphasized that IV conscious sedation is a practical alternative for the majority of advanced urologic procedures. However, careful patient selection is key to ensure a smooth and successful procedure.
While conscious sedation has gained prominence in urologic procedures, some urologists opt for a different approach. They prefer utilizing local anesthesia in combination with nitrous oxide to help patients relax during the procedure. This approach ensures safety and a stress-free experience for patients.
Why conscious sedation for urologic procedures is preferred
In conclusion, the study’s findings underscore the growing importance of conscious sedation as a preferred and safer alternative for urologic procedures. Patient comfort and safety are paramount, and the choice of anesthesia should be tailored to individual preferences and the specific nature of the procedure.

Hip fractures represent a significant and potentially life-threatening injury, with their likelihood increasing as individuals age. This elevated risk can be attributed to age-related bone weakening, often associated with osteoporosis. Furthermore, the use of multiple medications, coupled with issues like poor vision and balance problems, heightens the susceptibility of older individuals to falls, a common trigger for hip fractures. Managing a hip fracture typically involves surgical repair or replacement, followed by a course of physical therapy. Preventative actions aimed at maintaining bone density and reducing the risk of falls play a crucial role in averting hip fractures
Hip Fracture Patients Pain Experiences Study
In a recent study published in the Annals of Internal Medicine, researchers conducted a comparison of pain levels among patients who underwent hip fracture repair surgery, with a specific focus on those who received either spinal anesthesia or general anesthesia. The study, encompassing 1600 patients, yielded noteworthy findings regarding hip fracture patients and their post-surgical pain experiences.
Dr. Mark Neuman, the study’s lead author and an associate professor of anesthesiology and critical care at the University of Pennsylvania Perelman School of Medicine, highlighted the significance of this research. He pointed out that despite the longstanding use of both spinal and general anesthesia in hip fracture surgeries, there has been a notable lack of credible information concerning critical aspects of patient experience, notably pain and satisfaction following surgery. The study aimed to bridge this knowledge gap.
The initial study’s cohort comprised patients aged 50 and older who were scheduled for hip fracture surgery. Exclusion criteria included patients who were unable to walk without assistance prior to their fractures, those in need of concurrent procedures incompatible with spinal anesthesia, individuals with periprosthetic fractures, and those with contraindications to spinal anesthesia.
The study’s results revealed that hip fracture patients who received spinal anesthesia reported higher pain levels during the first 24 hours post-surgery compared to their counterparts who underwent general anesthesia. While the mean difference in pain scores was relatively modest, it was statistically significant.
Dr. Mark Neuman suggested one possible explanation for the observed differences between the two anesthesia groups. Patients who received spinal anesthesia received less opioid pain medication in the operating room, potentially contributing to the disparities in pain levels during the initial 24-hour period. However, more data is needed to draw definitive conclusions in this regard.
In an accompanying editorial commentary, Dr. Alexander Arriaga and Dr. Angela M. Bader of Brigham and Women’s Hospital in Boston, Massachusetts, commended the study for challenging the prevailing notion that spinal anesthesia might be more beneficial for hip fracture patients. Although the study’s authors had hypothesized that spinal anesthesia would result in less pain, reduced analgesic usage, and increased satisfaction with care, the actual findings did not align with these expectations.
However, Dr. Arriaga and Dr. Bader also noted that while the observed pain score differences were statistically significant, they were relatively small. This led them to question the clinical significance of such differences, considering that the absolute changes in pain scores were limited.
Both Dr. Neuman and Dr. Arriaga expressed concerns about the fact that more than 70% of patients in both anesthesia groups reported experiencing severe pain in the days immediately following surgery. They emphasized the need for additional research to delve into the underlying mechanisms of these differences between the two anesthesia methods.
Dr. Neuman expressed his hope that future studies will build upon the findings from this study to further investigate the connection between anesthesia type and crucial outcomes for hip fracture patients. This research was funded by a Patient-Centered Outcomes Research Institute award, and Dr. Arriaga disclosed no relevant financial relationships.


